Demodex Treatment: The Complete Step-by-Step Protocol
If you’ve been diagnosed with — or suspect — a Demodex overgrowth, the most common reason treatment fails isn’t the product you choose. It’s the approach. People treat for a week, see no change, and quit. Or they attack the mites so aggressively they damage their skin and make everything worse.
This guide lays out a complete, structured Demodex treatment protocol — the same four-phase logic clinicians use — explained clearly enough to follow at home and backed by the clinical evidence practitioners rely on.

Why most Demodex treatment fails
Demodex mites have a life cycle of roughly 14 to 18 days, from egg to larva to adult. This single fact explains most treatment failures: a course that lasts only a few days kills the adults present but does nothing about the eggs that hatch days later.
Effective treatment has to outlast several reproductive cycles. That’s why nearly every credible protocol runs a minimum of six weeks, often longer, with a maintenance phase afterward to prevent the population rebuilding. Patient compliance over this period is, by most clinical accounts, the biggest single predictor of success.
The core principle: Demodex treatment is a marathon, not a sprint. You’re not trying to win in three days — you’re outlasting the mite life cycle and then keeping numbers down. Consistency beats intensity every time.
Phase 1 — Confirm the diagnosis
Before treating, it’s worth confirming Demodex is actually the problem, because its symptoms overlap heavily with acne, rosacea, and ordinary dry skin. The standard clinical tool is the standardized skin surface biopsy (SSSB) — a quick, non-invasive sample taken from the cheek and examined under a microscope to count mites.
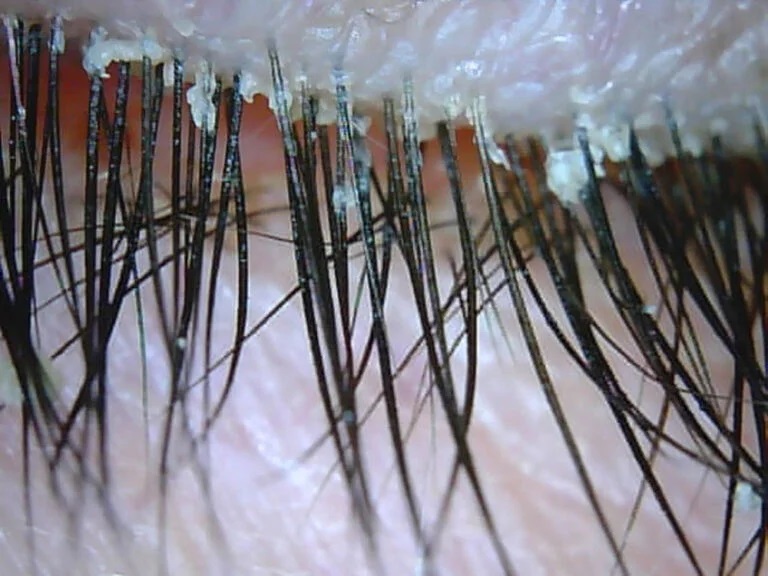
A density above roughly 5 mites/cm², combined with symptoms, supports a diagnosis of demodicosis. For eye involvement, clinicians look for collarettes — cylindrical cuffs at the base of the eyelashes, which are considered a hallmark sign. You can read the detail in our complete clinical guide to Demodex.
Phase 2 — The active kill phase
This is where mite numbers are brought down, using an acaricide — an agent that kills mites. Options range from natural to prescription, and the right choice depends on severity and location.
What the active phase involves
A topical acaricide applied consistently. For many mild-to-moderate cases this means a terpinen-4-ol (tea tree) based regimen; for others, a prescription agent such as topical ivermectin or metronidazole. The agent is applied to the whole affected area — not just visible spots — because mites move between follicles.
Tea tree oil’s active compound, terpinen-4-ol, has well-documented acaricidal activity; a systematic review of tea tree oil against ectoparasites supports its use against Demodex. For rosacea-associated cases, topical ivermectin has strong evidence, and a documented die-off reaction after ivermectin treatment illustrates how effective mite reduction can temporarily intensify symptoms before improvement.
Expect a possible flare. As large numbers of mites die, the immune response to their breakdown can briefly worsen redness, itching, or bumps. This “die-off” is often a sign the treatment is working — but a severe or rapidly spreading reaction, swelling, or signs of infection warrant stopping and seeing a clinician.
Phase 3 — Barrier repair
This phase is overlooked far too often. An intact skin barrier is one of your best defenses against mite overgrowth — and harsh treatment can damage it, creating the very environment Demodex thrives in.
Supporting the skin while you treat
Gentle, non-stripping cleansing. A barrier-supportive moisturizer. Daily SPF. Stepping back from unnecessary strong actives. The goal is to keep the skin calm and resilient so it can recover as mite numbers fall. See our guide to supporting your skin barrier and daily habits.
Phase 4 — Maintenance
Because Demodex are a normal part of human skin, the goal isn’t permanent elimination — it’s keeping the population in a healthy range so symptoms don’t return. After the active phase clears symptoms, most people drop to a lighter maintenance routine: a gentler frequency of the same acaricidal product, often two to three times a week, indefinitely or seasonally.
Don’t stop the moment your skin looks better. That’s exactly when mite numbers are lowest and the temptation to quit is highest — and it’s how relapses happen. Ease into maintenance rather than stopping cold. If you’re unsure how to taper, ask your clinician to map it out for your specific situation.
Treatment options compared
There’s no single “best” Demodex treatment — the right choice depends on severity, whether the eyes are involved, and your overall health. Here’s how the main categories compare.

For ocular Demodex specifically, the landscape changed in 2023: the American Academy of Ophthalmology notes lotilaner ophthalmic solution (Xdemvy) as the first FDA-approved treatment for Demodex blepharitis. Severe or immunocompromised cases may require oral ivermectin under medical supervision, while refractory cases sometimes benefit from in-office procedures like intense pulsed light (IPL) or microblepharoexfoliation.
Notes for clinicians
Diagnosis rests on SSSB with a threshold of >5 D. folliculorum/cm² plus clinical correlation. First-line topical options include terpinen-4-ol preparations and topical ivermectin or metronidazole; lotilaner is FDA-approved for Demodex blepharitis. Treatment should span multiple 14–18 day life cycles (minimum ~6 weeks) with a maintenance taper. Counsel patients on the self-limiting die-off reaction and on barrier preservation to avoid iatrogenic dermatitis.
The evidence base for Demodex management has matured considerably; DermNet’s overview of demodicosis provides a useful reference summary of acaricidal options including ivermectin, metronidazole, benzyl benzoate, and crotamiton, while emphasizing that asymptomatic colonization needs no treatment.
Looking for gentle, Demodex-supportive skincare?
demodex.net/ keeps an independent, standards-reviewed list of products.
Frequently asked questions
How long does Demodex treatment take?
Because the mite life cycle is roughly two to three weeks, most protocols run a minimum of six weeks, often longer, followed by ongoing maintenance. Stopping too early is the most common cause of relapse.
What is the most effective Demodex treatment?
It depends on the case. Terpinen-4-ol (tea tree) preparations work well for many mild-to-moderate cases; topical ivermectin or metronidazole are common for rosacea overlap; lotilaner is FDA-approved for eye involvement. Severe cases may need oral ivermectin. The best results usually come from a structured, sustained protocol rather than any single product.
Can Demodex be cured permanently?
Demodex mites are a normal part of human skin, so the realistic goal is control rather than total eradication. Maintenance care keeps numbers low enough that symptoms don’t return.
Why did my skin get worse after starting treatment?
This is often a “die-off” reaction — the immune response to large numbers of dying mites — and frequently a sign treatment is working. However, severe swelling, spreading rash, or signs of infection are not typical and warrant medical review.
References
- DermNet. Demodex and demodicosis. dermnetnz.org/topics/demodex
- Bezabh SA, et al. Antiparasitic activity of tea tree oil (TTO) and its components against medically important ectoparasites: a systematic review. Pharmaceutics. 2022;14(8):1587. pubmed.ncbi.nlm.nih.gov/35893684
- Die-off reaction of Demodex mites after treating demodicosis with oral ivermectin: a case report. PMC. ncbi.nlm.nih.gov/pmc/articles/PMC11399466
- American Academy of Ophthalmology. Demodex: friendly commensal or fiendish foe? aao.org
- Forton F, et al. Demodicosis and rosacea: epidemiology and significance in daily dermatologic practice. J Am Acad Dermatol. 2005;52(1):74–87.
Medical disclaimer: This article is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Prescription treatments require medical supervision. Always consult a qualified healthcare provider, particularly for eye symptoms or if you are immunocompromised. demodex.net/ is an independent educational resource and does not provide medical diagnoses.